


Dempsey Wood BSc1*, Keith Da Silva DDS, MSc1
1College of Dentistry, University of Saskatchewan, Saskatoon, Canada
Corresponding author:
Dempsey Wood
105 Wiggins Road
Saskatoon, SK, S7N 5E4, Canada
Email: Dww533@usask.ca
ABSTRACT
Background: The COVID-19 pandemic was a challenge for all dental professionals who had to rapidly update infection prevention and control (IPAC) guidelines and protocols due to increased risk of SARS-CoV-2 transmission during common aerosol-generating procedures (AGPs), and a lack of consensus on how best to mitigate the risk of transmission in a dental office. Thus, the purpose of this descriptive study was to compare the variance in IPAC guidelines for dental offices that emerged, and to assess practice consistency from early to mid-2020.
Methods: A comprehensive literature search was conducted from May 26 to July 8, 2020 for IPAC documentation specific to the dental office during the COVID-19 pandemic. Documents that met the inclusion criteria were independently reviewed. Data was extracted using a framework based on the following IPAC domains:
pre-appointment, waiting room, personal protective equipment (PPE) selection, treatment room, and post-dismissal.
Results: A total of 67 IPAC documents specific to dental offices were reviewed in this study. Included documents originated from 22 dental associations, 17 peer-reviewed articles, 13 dental regulators, 11 government bodies, two public health units, and two dental corporations. There was a great degree of variance with IPAC guidelines from the pre-appointment stage, during treatment, and post-treatment. Recommendations that emerged with some level of consistency involved pre-screening patients for COVID-19 symptoms (97%), staggering appointments (84%), social distancing, minimizing occupants in the waiting room, wearing a face shield over protective eyewear for AGPs (92%), and preprocedural rinses (84%). There was less consistency with recommendations for consolidating multiple appointments (36%), waiting room ventilation (46%), N95 masks (47%) versus FFP2/FFP3 masks (30%) use for AGPs, fit-testing respirators (37%), enclosing open operatories for AGPs (28%), prioritizing minimally invasive procedures (30%), and using third-party laundry companies (32%).
Conclusions: The risk of SARS-CoV-2 transmission, lack of consensus on mode of spread, and need for rapid action resulted in a significant variation in most downstream IPAC interventions in the hierarchy of controls, including choice of PPE, treatment room, and post-dismissal domains. Upstream interventions, including pre-appointment and waiting room domains, were relatively consistent in practices in early to mid-2020.
KEYWORDS: aerosols, COVID-19, dentistry, guideline, infection control
INTRODUCTION
The coronavirus disease (COVID-19) was first identified in Wuhan, China in December, 2019 after a group of patients presented to the hospital with atypical pneumonia [1]. Evolving transmission patterns of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and elusive variants have challenged public health strategies and prolonged the pandemic [2]. SARS-CoV-2 can be transmitted by direct contact with contaminated surfaces, contact with discharge from nose or mouth, and most commonly via droplet dispersion when an infected person coughs, sneezes, or undergoes an aerosol-generating procedure (AGP) [3]. Most dental procedures generate aerosols that are contaminated with a patient’s saliva, blood, secretions, or tissue particles [4]. Due to increased transmission risks during dental AGPs, dental treatment in most countries across the world was paused and limited to emergency care in the early stages of the pandemic [3]. Dental clinics gradually re-opened in phases under strict infection prevention and control (IPAC) guidelines mandated by public health authorities and dental regulators. Each authority responsible for creating guidelines had to review new information as it became available and update their guidelines.
Considering the proximity of dental care providers (DCPs) to patients during treatment and the contamination and spread of aerosols, dental offices were considered to be a high-risk setting for COVID-19 transmission [5]. The disease can readily spread from infected patients to the DCPs, to other patients and vice versa without appropriate IPAC protocols. Longstanding measures include personal protective equipment (PPE), hand hygiene, proper equipment handling and sterilization, procedural risk reduction, and disinfection and sterilization protocols [6]. Considering the risk of transmission of COVID-19 in dental settings, dental professionals had to re-evaluate the entire dental continuum of care, including tracking patients through the entire array of dental services from pre-appointment, waiting room, PPE selection, treatment room, and post-dismissal. Guidelines demanded that offices were redesigned to accommodate social distancing, minimize contact points, and conform with overarching public health mandates.
Since it is imperative that dental offices adapt strategies to mitigate the spread of COVID-19 aerosols, in this study, we reviewed interventions for consistency. In the dental setting, droplets from AGPs can reach the DCP’s eyes and nose, which could increase the likelihood of SARS-CoV-2 transmission [7,8]. Particulate respirators filter out 0.1 to 0.3 micron particles during AGPs [9]. Protective eyewear and face shields may prevent infectious droplets from contaminating conjunctival epithelium [10]. Hydrogen peroxide (HP), chlorhexidine (CHX), and povidone iodine (PI) preprocedural rinses (PPRs) may reduce viral loads of SARS-CoV-2 in saliva and oropharyngeal tissues, and consequently in aerosols [11–13]. Aerosol transmission can be mitigated at the source via rubber dam isolation, high-volume evacuation and allowing a “fallow time” for air circulation and droplet settling [14].
As information on the transmission and epidemiology of COVID-19 continues to evolve, policymakers interpret scarce scientific evidence and changing advice from international health agencies to develop guidelines for safe delivery of oral healthcare services. A rapidly evolving understanding of the infectiousness and transmissibility of COVID-19, scarce evidence supporting novel IPAC measures in dental offices, and unique risk of acquiring COVID-19 via aerosol created the “perfect storm” for inconsistent recommendations. Thus, the aim of this study was to identify variance in IPAC guidelines specific to dental offices in early to mid-2020 of the COVID-19 pandemic, from pre-appointment, waiting room, PPE selection, treatment room, and post-dismissal.
METHODS
A comprehensive search for IPAC documents specific to dental offices during the COVID-19 pandemic was conducted by an independent reviewer (DW) between May 26, 2020, and July 8, 2020. Both authors (KD and DW) independently reviewed documents to create a mutually agreed upon inclusion list. Inclusion criteria included English language guidance documents by professional bodies for dentists, guidance from national or subnational (i.e., province or state) bodies, peer-reviewed scientific publications, guidance for resuming or maintaining dental practice during the COVID-19 pandemic, guidance for the entire continuum of dental care from pre-appointment, waiting room, treatment room, and post-dismissal. Consensus statements, guidance for dental auxiliaries, local (i.e., town, city, or county) guidance and sources exclusively focusing on select recommendations, or not specific to dentistry were excluded.
A search for IPAC documents and publications was conducted using the following databases: MEDLINE, EMBASE, Scopus, Cochrane Library, and Google Scholar. The following terms and Boolean operators were used in MeSH and free-text searches: OR infection OR prevention and OR control, OR emergency, OR urgent, OR non-urgent, AND dental OR settings, OR oral OR health OR services, OR IPAC, OR interim, OR phase 1, OR phase 2, OR phase 3, OR plan, OR procedure, OR guidance, OR guideline, OR return, OR recovery, OR practice, OR dentistry, OR covid-19, and OR return to work. Additionally, a search of the grey literature was conducted to identify IPAC documents produced directly by dental associations, regulatory bodies, and governing health authorities.
Eligible IPAC documents were reviewed and the following document elements were first extracted: country/region of publisher, organization name, type of organization (i.e., health authority, dental association, dental regulator), document title, language, document URL, date published, date updated, and whether or not it was a live document (Supplementary Table 1). A framework for extracting IPAC content was developed in advance based on the following stages of patient flow through an office: pre-appointment, waiting room, treatment room, and post-dismissal. The collected data was organized according to theme, and descriptive data is reported. The proportion (%) of each individual recommendation category was calculated by relating frequency to total number of guidelines.
RESULTS
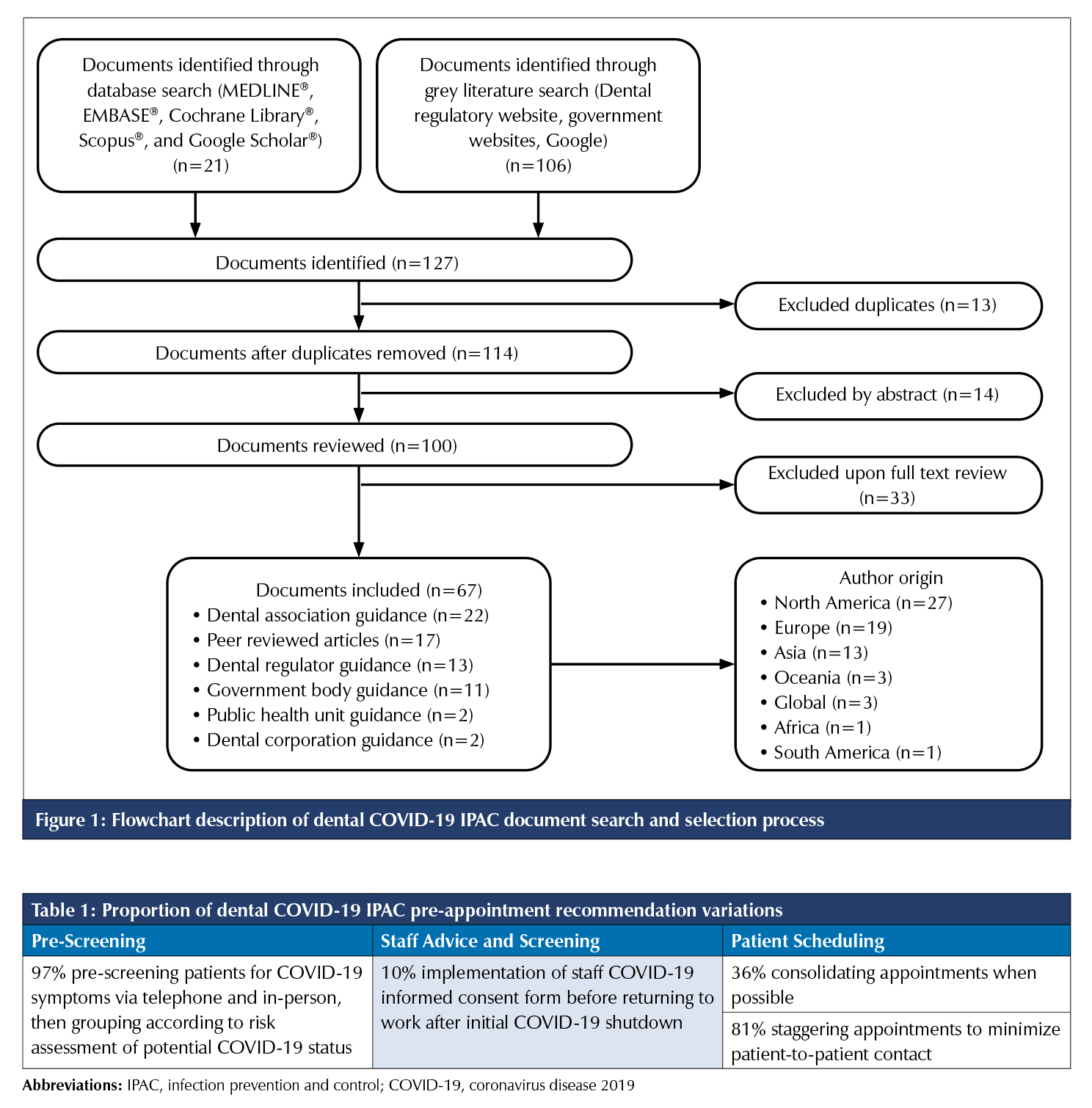
Recommendations were summarized according to frequency of recommendation variations and proportion of sources represented for patient flow categories. The initial search identified 127 documents; 100 documents were fully reviewed, and 67 guidance documents were selected after exclusions. The full review of search process is described in Figure 1.
Pre-Appointment
A summary of pre-appointment recommendations is presented in Table 1. Almost all (97%) guidelines recommended pre-screening patients and temporally scheduling according to COVID-19 risk. Interestingly, only 10% of the guidelines reviewed recommended implementing a COVID-19 staff informed consent form prior to returning to work after the initial COVID-19 shutdown. The purpose of the form was to make staff aware of the risks involved upon returning and working during the COVID-19 pandemic. The majority (81%) of guidelines recommended staggering appointments to minimize patient-to-patient contact and 36% recommended combining appointments when possible.
Waiting Room
A description of recommendations specific to dental office waiting rooms is presented in Table 2. Most guidelines (88%) adopted local public health recommendations for the waiting room such as social distancing, hand hygiene, and minimizing contact points. A total of 83% of sources recommended installation of a clear plastic barrier at the reception desk. Ninety-two percent of sources recommended minimizing occupants to allow for social distancing – most of these sources recommended social distancing of at least two metre (72%), while others recommended one metre (22%). Less than half (46%) of the guidelines recommended improving airflow in the waiting room, either by opening windows or using air-filtration systems. Almost all guidelines promoted passive screening, including requirements for patient hygiene (92%), and placement of COVID-19 information posters (81%).
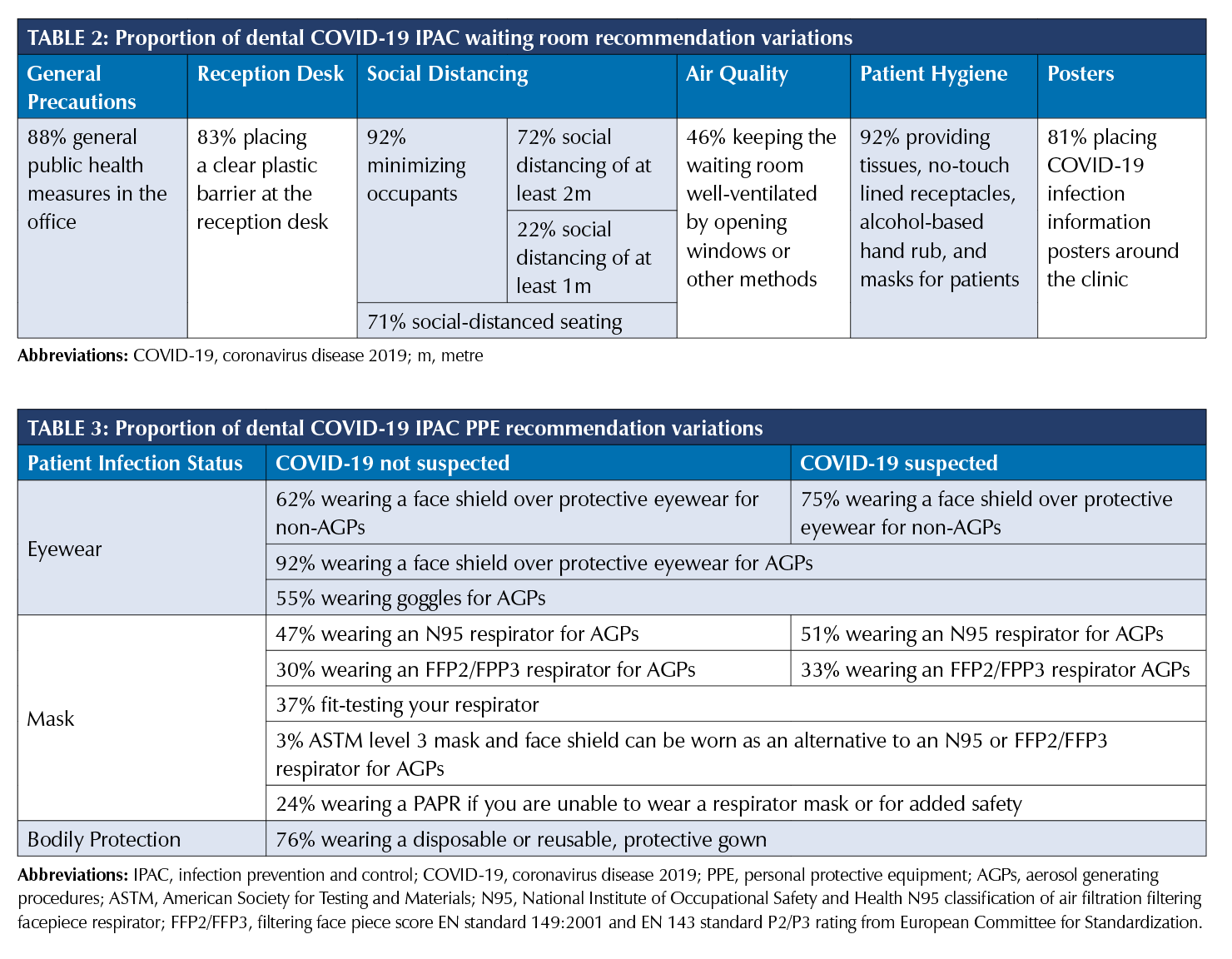
Personal Protective Equipment
A summary of relevant PPE recommendations is presented in Table 3. PPE recommendations were stratified based on COVID‑19 infection status of patients and type of procedure (AGP or non-AGP). Only 62% of sources recommended wearing an additional face shield over protective eyewear for non-AGPs on unsuspected COVID-19 patients. Conversely, for AGPs, the large majority (92%) of sources recommended wearing a face shield over protective eyewear for all patients. Very few (3%) sources considered an American Society for Testing and Materials (ASTM) level 3 mask and face shield as an alternative to a 95% filtration efficiency respirator (N95) or filtering facepiece class 2 or 3 (FFP2/FFP3) for AGPs. Only 37% of sources required that respirators are fit-tested prior to use. Over half (51%) of sources recommended wearing an N95 respirator and only a third (33%) of the guidelines recommended wearing an FFP2 or FFP3 respirator for AGPs on suspected COVID-19 patients. More than three-quarters (76%) of sources recommended wearing a protective gown for bodily protection during all procedures.
Treatment room
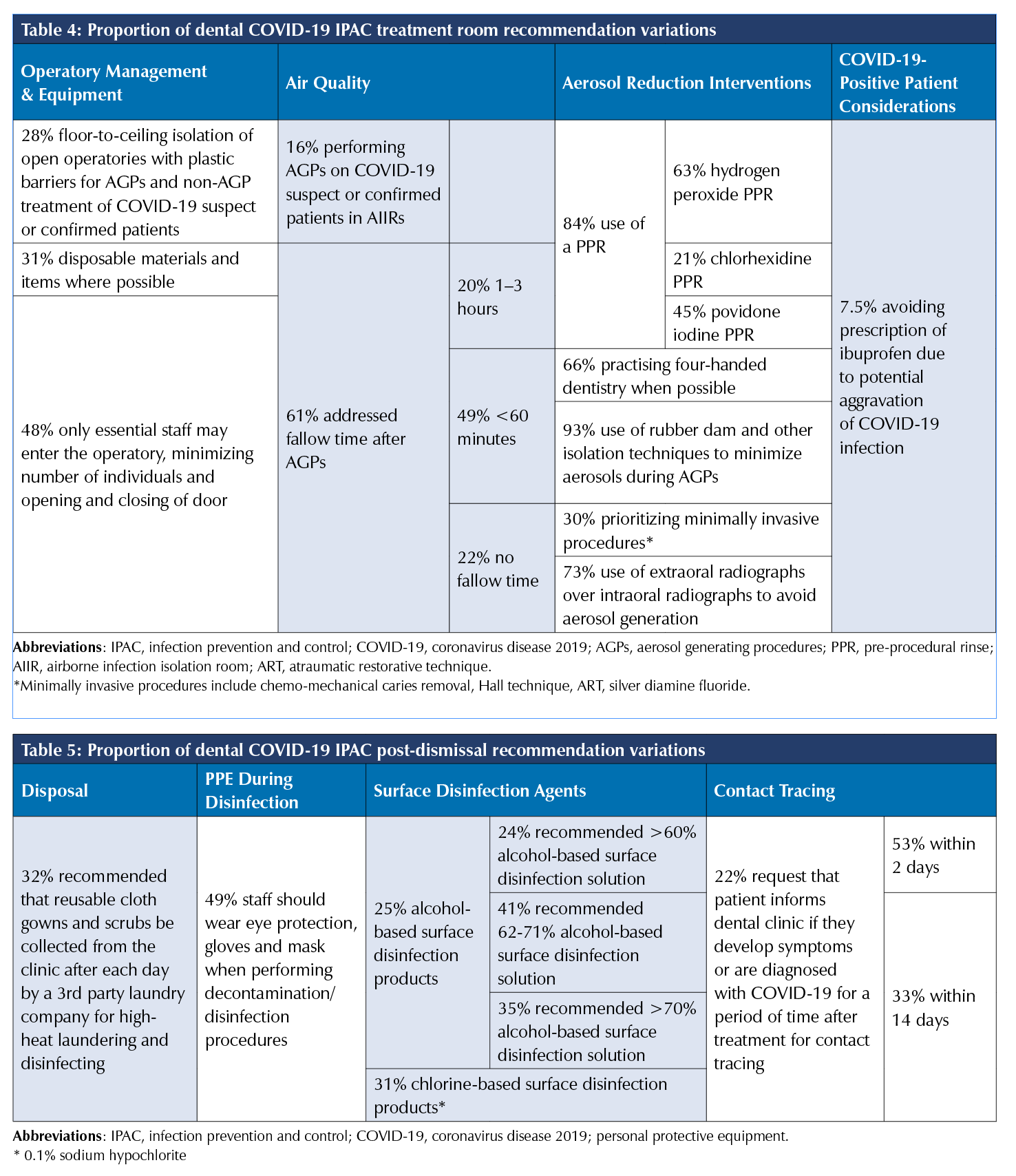
IPAC recommendations for treatment rooms and during procedures are presented in Table 4. Select sources (28%) mandated separation of operatories with plastic barriers (from floor-to-ceiling) for AGPs for suspected or confirmed patients with COVID-19. Very limited sources (16%) required AGPs on COVID-19 patients to be completed in airborne infection isolations rooms (AIIRs). Sixty-one percent of sources addressed fallow time after AGPs. Of these sources, about half recommended (49%) a fallow time of less than 60 minutes, some (20%) recommended a fallow time of 1–3 hours, and others (22%) specifically stated that a fallow time was not required. There was widespread (84%) agreement for PPRs, most commonly (63%) recommending an HP rinse, followed by PI (45%). About two thirds (66%) of sources recommended practicing with an assistant at all times for constant use of high-volume suction, often denoted as “four-handed dentistry”. Most (93%) guidelines emphasized the importance of utilizing a rubber dam and other isolation techniques such as PVS‑based isolation pastes, cotton rolls and gauze, and cheek retraction suction devices. Only 30% of sources recommended prioritizing minimally invasive operative procedures such as chemo-mechanical caries removal, Hall technique, atraumatic restorative technique (ART), or silver diamine fluoride. Very few (7.5%) sources recommended avoiding prescription of ibuprofen due to potential aggravation of COVID-19 infection.
Post-Dismissal
A summary of post-dismissal recommendations of interest is listed in Table 5. About one-third (32%) of sources recommended daily collection of reusable gowns and scrubs by a third-party laundering service. About half (49%) of sources recommended that staff wear standard PPE during disinfection/decontamination procedures, including eyewear, gloves, and mask. Of sources that recommend alcohol-based surface disinfection products (25%), a 62-71% alcohol-based surface solution was most frequently recommended (41%). Some guidelines (22%) asked that patients inform the clinic if they develop symptoms, or are diagnosed with COVID‑19 after treatment for contact tracing and isolation of close contacts. Of these, 53% required follow-up after two days, and 33% for 14 days.
Discussion
This study compares and contrasts the different IPAC guidelines that emerged specific for dental offices during the COVID‑19 pandemic for pre-appointment, waiting room, PPE use, treatment room, and post-dismissal domains. Among 67 guidelines included, various recommendations were homogeneous in each category. This includes pre-appointment recommendations such as pre-screening and staggering appointments and waiting room recommendations such as social distanced seating, hand hygiene, and COVID-19 information posters. Most pre-appointment and waiting room recommendations were not specific to the dental environment and matched overarching public health guidelines that were relatively consistent internationally. There was agreement in PPE choice, treatment room, and post-dismissal measures supported by evidence available at the onset of the pandemic. Both cost-effective and reusable, face shields were uniformly recommended for AGPs. Face shields have been shown to reduce immediate viral exposure by 68-96% during AGPs [15]. Wearing a disposable or reusable protective gown was also widely recommended, and shown to be effective in reducing infection rate [16,17]. Treatment room guidelines were most alike in recommending a fallow time of less than 60 minutes, which preliminary evidence supports, including the use of PPRs [18,19]. Similarities existed in post-dismissal recommendations for the use of 62-71% ethanol disinfectant, that has been shown to rapidly inactivate human coronaviruses in experimental studies, and intuitive use of eye protection, gloves, and mask during disinfection [13].
Widespread agreement in recommending PPRs can be accounted for by the pre-existing body of literature available demonstrating their effectiveness in significantly reducing microbes in dental aerosols [20]. Three of the most recommended rinses include HP, PI, and CHX. However, the majority of studies referenced evaluated microbial loads using colony-forming units, which excludes viruses [11,21–25].
Hypothetical inferences were made from the available research demonstrating that these PPRs reduced aerosol loads of other enveloped viruses in different capacities, depending on concentration and duration of use [20,26]. More recently, PI was shown to completely deactivate SARS-CoV-2 after 15 seconds in-vitro and reduced salivary viral load up to six hours after use in COVID-19 positive patients [27,28]. PI may not be most commonly recommended because of infrequent adverse events reported such as burning sensation, itching, and local irritation [29]. CHX was least frequently recommended by sources, reflected by sparing evidence showing conflicting efficacy – further studies are needed to support its use [20]. HP is supported by few studies showing its ability to inactivate microbes at low, non-toxic concentrations (0.5-3%) after 30-60 seconds of use [13]. A recent in-vitro study demonstrated some success in inactivating SARS-CoV-2, but a pilot study of ten COVID-19 positive patients did not find a significant reduction [13,30]. Differences in cost may have also impacted rinse recommendations. Randomized controlled trials with large sample sizes are required to evaluate effectiveness of PPRs against SARS-CoV-2. The potential of PPRs to significantly reduce risk of aerosol transmission, and ease of implementation suggests that PPRs should remain within standard operating procedures (SOPs) going forward.
Guideline recommendations unique to dentistry differed in abundance. While the majority of sources adopted a social distance measure of two metres, there were still some recommendations for a shorter distance of one metre, which is likely explained by local differences in public health orders. Evidence suggests SARS-CoV-2 may travel more than 2m through coughing and shouting [31]. Stark differences in PPE recommendations were noted for respiratory hygiene; N95 respirators during AGPs versus FFP2/FFP3 respirators despite similar filtration efficiency [9]. This can be explained by geographic standardization of N95s in North America and FFP2/FFP3s in Europe [9]. Only few advocated for fit-testing respirators as this may have been included in general healthcare service guidelines that encompassed DCPs, as it has been established that fit-testing increases protective factors offered by respirators [32].
Lack of consensus surrounding aerosol transmission of COVID-19 and limited research on dental AGP's resulted in significant variance in suggestions for air control in operatories. Fallow time also depends on each unique facility’s air circulation variables, complicating recommendations [14]. Only 22% of guidelines stated that a fallow time was not required after AGPs. The effectiveness of fallow time may have been overstated early in the pandemic. A recent study suggested that intraoral high-volume suction alone or in combination with other air-cleaning methods reduced particle concentrations to baseline on completion of AGPs and may negate need for fallow time [4]. Those responsible for drafting guidelines likely looked to professional agencies like the CDC and/or WHO for early IPAC guidance because of insufficient experimental evidence about COVID-19. CDC guidelines recommended that practices determine fallow times using NIOSH’s mathematical relationship for rate of decline in concentration of airborne contaminant [33]. This hypothetical model assumes the aerosolized environment is an empty room with ideal mixing of room air after the contaminant source is removed [14].
Minimally invasive restorative procedures, which would not generate aerosols, were not frequently endorsed. However, most guidelines did recommend avoiding AGPs when possible. Beyond the benefit of conserving tooth structure, clinicians may opt for evidence-based, minimally invasive procedures more frequently for the management of caries because they reduce or eliminate aerosol transmission [34]. Only five sources recommended avoiding the prescription of ibuprofen after a letter published in the Lancet on March 11, 2020 hypothesized that ibuprofen may aggravate COVID‑19 symptoms [35]. Shortly after, a retrospective cohort study by Rinott et al. showed that ibuprofen was not associated with worse clinical outcomes [36]. Most sources did not recommend professional out-of-house laundering potentially due to controversy in the literature on whether soiled linen risks disease transmission. The CDC stated that it presents a negligible risk for infection and normal ‘hot’ and ‘cold’ washing-drying cycles are adequate for patient safety.” While the Association of Surgical Technologists recommended professional laundering due to the extent of contamination [37]. This is an opportunity for practice leaders to review dress code policies to ensure safety for patients and providers. Introducing research opportunities for how different aspects of scrubs may impact contamination (i.e., material and duration of use). The dichotomous difference in contact tracing recommendations between two and 14 days can be explained by national differences in public health protocols post-confirmation and ambiguity in the virus’ infectious period [38].
The potential airborne nature of COVID-19 and ability to rapidly disseminate demanded that decision-makers revamp protocols to include overriding public health measures. Simultaneously, guideline creators had to address dental-specific concerns of COVID-19, namely AGPs. The need to define dental AGPs in guidelines created ambiguity, however, the use of high-speed handpieces, air-water syringes, and ultrasonic scalers were consistently considered AGPs [39]. Virdi et al. found that risk stratification of COVID-19 transmission associated with different AGPs was inconsistent among early guidelines, but guidelines released later were more descriptive [39]. During initial reopening, it may have been rational to expect inconsistent guidelines for a novel viral pathogen; evidence consulted was likely based on rapid reviews and mixed findings from published data. To fill this gap, current research has focused on many of these uncertainties resulting in rapid production of a large volume of literature [40]. Bibliometric analysis by Jacimovic et al. analyzing 296 dental COVID-19 studies identified a low overall level of scientific evidence [40]. The authors concluded that current literature does not provide sufficient data for the evidence-based decision-making process required for guiding clinical practice [40]. It will be important to thoroughly analyze the vast COVID-19 scientific evidence available to corroborate new findings specific to dentistry.
Robust IPAC protocols existed in dentistry prior to the pandemic but the uncertainty with regards to infectivity and transmissibility of the virus challenged norms. Importance placed on IPAC in dental settings can be appreciated by the lack of super-spreader events involving dental practices in the literature [33]. Following the precautionary principle, in the absence of definitive scientific evidence on how to prevent transmission in a dental office, policymakers and dental regulators had to err on the side of caution to protect the public. The level of caution dental authorities took to account for growing uncertainty and complexity reflects itself in the variety of different guidelines observed. Current guidelines have not changed significantly, but have only become more lenient. Identifying variations in guidelines emphasizes where high-quality evidence is needed to determine efficacy of cross-infection interventions for delivery of safe oral health care in a post-pandemic world. Clinical studies are needed to elucidate which new measures accurately reduce infection risk without trade-offs of time spent with patients and expense, facilitating creation of uniform, practical IPAC guidelines.
The findings of this study are strengthened by a broad search criteria used to capture guidelines and recommendations published outside academic literature. With a data collection period over three months, updated guidelines were captured in real-time as new information became available. However, it is important to consider the limitations of this research. Only guidelines in English language were considered. Although translated documents were accessible for various European and Asian countries, this was not always the case. Frequency of certain recommendations may have been understated if they were only captured in multidisciplinary or broad public health orders that offices adhered to. There have been considerable developments since initial search in early to mid-2020, such as ventilation and engineering controls, vaccinations, and variants of concern that are not reflected in this study.
CONCLUSION
Due to the transmissibility of the SARS-CoV-2 virus, limited evidence, and short time period to act, our study demonstrates a considerable variation in downstream IPAC recommendations specific to dental offices in the domains related to PPE choice, treatment room, and post-dismissal recommendations. Upstream interventions that focused on eliminating exposure through pre-appointments and precautions in the waiting room were fairly consistent across guidelines. While pre-COVID-19 IPAC guidelines for dental offices were once considered robust, this pandemic revealed areas that need to be addressed in the post-pandemic world. Moving forward, a greater emphasis needs to be placed on developing evidence-based IPAC guidelines that will allow dental professionals to provide safe and effective treatment.
REFERENCES
(1) Allam, Z. (2020). The First 50 days of COVID-19: A Detailed Chronological Timeline and Extensive Review of Literature Documenting the Pandemic. Surveying the Covid-19 Pandemic and Its Implications, 1–7. https://doi.org/10.1016/B978-0-12-824313-8.00001-2.
(2) Kaur, N., Singh, R., Dar, Z., Bijarnia, R. K., Dhingra, N., & Kaur, T. (2021). Genetic comparison among various coronavirus strains for the identification of potential vaccine targets of SARS-CoV2. Infection, Genetics and Evolution, 89, 104490. https://doi.org/10.1016/j.meegid.2020.104490.
(3) Peng, X., Xu, X., Li, Y., Cheng, L., Zhou, X., & Ren, B. (2020). Transmission routes of 2019-nCoV and controls in dental practice. International Journal of Oral Science, 12(1), 1–6. https://doi.org/10.1038/s41368-020-0075-9.
(4) Ehtezazi, T., Evans, D. G., Jenkinson, I. D., Evans, P. A., Vadgama, V. J., Vadgama, J., Jarad, F., Grey, N., & Chilcott, R. P. (2021). SARS-CoV-2: Characterisation and mitigation of risks associated with aerosol generating procedures in dental practices. British Dental Journal, 1–7. https://doi.org/10.1038/s41415-020-2504-8.
(5) Zhang, M. (2021). Estimation of differential occupational risk of COVID-19 by comparing risk factors with case data by occupational group. American Journal of Industrial Medicine, 64(1), 39–47. https://doi.org/10.1002/ajim.23199.
(6) Brondani, M., Cua, D., Maragha, T., Shayanfar, M., Mathu-Muju, K., Bergmann, H. von, Almeida, F., Villanueva, J., Alvarado, A. A. V., Learey, S., & Donnelly, L. (2020). A Pan-Canadian narrative review on the protocols for reopening dental services during the COVID-19 pandemic. BMC Oral Health, 20(1), 1–13. https://doi.org/10.1186/s12903-020-01340-y.
(7) Nejatidanesh, F., Khosravi, Z., Goroohi, H., Badrian, H., & Savabi, O. (2013). Risk of Contamination of Different Areas of Dentist’s Face During Dental Practices. International Journal of Preventive Medicine, 4(5), 611–615.
(8) Bentley, C. D.; Burkhart, N. W.; Crawford, J. J. Evaluating Spatter and Aerosol Contamination during Dental Procedures. J Am Dent Assoc 1994, 125 (5), 579–584. https://doi.org/10.14219/jada.archive.1994.0093.
(9) Rengasamy, S., Eimer, B. C., & Shaffer, R. E. (2009). Comparison of Nanoparticle Filtration Performance of NIOSH-approved and CE-Marked Particulate Filtering Facepiece Respirators. The Annals of Occupational Hygiene, 53(2), 117–128. https://doi.org/10.1093/annhyg/men086.
(10) Lu, C., Liu, X., & Jia, Z. (2020). 2019-nCoV transmission through the ocular surface must not be ignored. The Lancet, 395(10224), e39. https://doi.org/10.1016/S0140-6736(20)30313-5.
(11) Reddy, S., Prasad, M. G. S., Kaul, S., Satish, K., Kakarala, S., & Bhowmik, N. (2012). Efficacy of 0.2% tempered chlorhexidine as a pre-procedural mouth rinse: A clinical study. Journal of Indian Society of Periodontology, 16(2), 213–217. Scopus. https://doi.org/10.4103/0972-124X.99264.
(12) Eggers, M., Koburger-Janssen, T., Eickmann, M., & Zorn, J. (2018). In Vitro Bactericidal and Virucidal Efficacy of Povidone-Iodine Gargle/Mouthwash Against Respiratory and Oral Tract Pathogens. Infectious Diseases and Therapy, 7(2), 249–259. https://doi.org/10.1007/s40121-018-0200-7.
(13) Kampf, G., Todt, D., Pfaender, S., & Steinmann, E. (2020). Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. The Journal of Hospital Infection, 104(3), 246–251. https://doi.org/10.1016/j.jhin.2020.01.022.
(14) Singhal, S., Farmer, J., Aggarwal, A., Kim, J., & Quiñonez, C. (2021). A Review of “Optimal Fallow Period” Guidance Across Canadian Jurisdictions. International Dental Journal. https://doi.org/10.1016/j.identj.2021.03.003.
(15) Lindsley, W. G., Noti, J. D., Blachere, F. M., Szalajda, J. V., & Beezhold, D. H. (2014). Efficacy of face shields against cough aerosol droplets from a cough simulator. Journal of Occupational and Environmental Hygiene, 11(8), 509–518. https://doi.org/10.1080/15459624.2013.877591.
(16) Madge, P., Paton, J. Y., McColl, J. H., & Mackie, P. L. (1992). Prospective controlled study of four infection-control procedures to prevent nosocomial infection with respiratory syncytial virus. Lancet (London, England), 340(8827), 1079–1083. https://doi.org/10.1016/0140-6736(92)93088-5.
(17) Srinivasan, A., Song, X., Ross, T., Merz, W., Brower, R., & Perl, T. M. (2002). A prospective study to determine whether cover gowns in addition to gloves decrease nosocomial transmission of vancomycin-resistant enterococci in an intensive care unit. Infection Control and Hospital Epidemiology, 23(8), 424–428. https://doi.org/10.1086/502079.
(18) Bates, A. J., & Bates, D. R. (2020). Analysing air particle quantity in a dental primary care setting. MedRxiv, 2020.08.12.20173450. https://doi.org/10.1101/2020.08.12.20173450.
(19) Haigh, A., Vasant, R., & O’Hooley, D. (2020). Quantitative evaluation of dental bio-aerosols using particle count values. Part 1: The effect of high-volume aspiration and natural ventilation. [Preprint]. Research Square. https://doi.org/10.21203/rs.3.rs-55265/v1.
(20) Marui, V. C., Souto, M. L. S., Rovai, E. S., Romito, G. A., Chambrone, L., & Pannuti, C. M. (2019). Efficacy of preprocedural mouthrinses in the reduction of microorganisms in aerosol: A systematic review. The Journal of the American Dental Association, 150(12), 1015-1026.e1. https://doi.org/10.1016/j.adaj.2019.06.024.
(21) Feres, M., Figueiredo, L. C., Faveri, M., Stewart, B., & de Vizio, W. (2010). The Effectiveness of a Preprocedural Mouthrinse Containing Cetylpyridinium Chloride in Reducing Bacteria in the Dental Office. The Journal of the American Dental Association, 141(4), 415–422. https://doi.org/10.14219/jada.archive.2010.0193.
(22) Gupta, G., Mitra, D., Ashok, K. P., Gupta, A., Soni, S., Ahmed, S., & Arya, A. (2014). Efficacy of Preprocedural Mouth Rinsing in Reducing Aerosol Contamination Produced by Ultrasonic Scaler: A Pilot Study. Journal of Periodontology, 85(4), 562–568. https://doi.org/10.1902/jop.2013.120616.
(23) Shetty, S. K., Sharath, K., Shenoy, S., Sreekumar, C., Shetty, R. N., & Biju, T. (2013). Compare the Efficacy of Two Commercially Available Mouthrinses in reducing Viable Bacterial Count in Dental Aerosol produced during Ultrasonic Scaling when used as a Preprocedural Rinse. The Journal of Contemporary Dental Practice, 14(5), 848–851. https://doi.org/10.5005/jp-journals-10024-1414.
(24) Dawson, M., Soro, V., Dymock, D., Price, R., Griffiths, H., Dudding, T., Sandy, J. R., & Ireland, A. J. (2016). Microbiological assessment of aerosol generated during debond of fixed orthodontic appliances. American Journal of Orthodontics and Dentofacial Orthopedics, 150(5), 831–838. https://doi.org/10.1016/j.ajodo.2016.04.022.
(25) Retamal-Valdes, B., Soares, G. M., Stewart, B., Figueiredo, L. C., Faveri, M., Miller, S., Zhang, Y. P., & Feres, M. (2017). Effectiveness of a pre-procedural mouthwash in reducing bacteria in dental aerosols: Randomized clinical trial. Brazilian Oral Research, 31, e21. Scopus.
https://doi.org/10.1590/1807-3107BOR-2017.vol31.0021.
(26) Reis, I. N. R., do Amaral, G. C. L. S., Mendoza, A. A. H., das Graças, Y. T., Mendes-Correa, M. C., Romito, G. A., & Pannuti, C. M. (2021). Can preprocedural mouthrinses reduce SARS-CoV-2 load in dental aerosols? Medical Hypotheses, 146, 110436. https://doi.org/10.1016/j.mehy.2020.110436.
(27) Bidra, A. S., Pelletier, J. S., Westover, J. B., Frank, S., Brown, S. M., & Tessema, B. (2020). Rapid In-Vitro Inactivation of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Using Povidone-Iodine Oral Antiseptic Rinse. Journal of Prosthodontics: Official Journal of the American College of Prosthodontists, 29(6), 529–533. https://doi.org/10.1111/jopr.13209.
(28) Singh, G. P., Vivekananda, L., & Roy, P. (2021). Effect of preprocedural oral rinses with active ingredients like chlorhexidine, povidone-iodine and cetylpyridinium chloride in neutralizing SARS-COV-2 concentration in aerosol. GSC Advanced Research and Reviews, 6(3), 132–135. https://doi.org/10.30574/gscarr.2021.6.3.0048.
(29) Olson, A. S., Rosenblatt, L., Salerno, N., Odette, J., Ren, R., Emanuel, T., Michalek, J., Liu, Q., Du, L., Jahangir, K., & Schmitz, G. R. (2019). Pilot Study to Evaluate the Adjunct Use of a Povidone-Iodine Topical Antiseptic in Patients with Soft Tissue Abscesses. The Journal of Emergency Medicine, 56(4), 405–412. https://doi.org/10.1016/j.jemermed.2018.12.026.
(30) Gottsauner, M. J., Michaelides, I., Schmidt, B., Scholz, K. J., Buchalla, W., Widbiller, M., Hitzenbichler, F., Ettl, T., Reichert, T. E., Bohr, C., Vielsmeier, V., & Cieplik, F. (2020). A prospective clinical pilot study on the effects of a hydrogen peroxide mouthrinse on the intraoral viral load of SARS-CoV-2. Clinical Oral Investigations, 24(10), 3707–3713. https://doi.org/10.1007/s00784-020-03549-1.
(31) Jones, N. R., Qureshi, Z. U., Temple, R. J., Larwood, J. P. J., Greenhalgh, T., & Bourouiba, L. (2020). Two metres or one: What is the evidence for physical distancing in Covid-19? BMJ, 370, m3223. https://doi.org/10.1136/bmj.m3223.
(32) Reponen, T., Lee, S.-A., Grinshpun, S. A., Johnson, E., & McKay, R. (2011). Effect of fit testing on the protection offered by n95 filtering facepiece respirators against fine particles in a laboratory setting. The Annals of Occupational Hygiene, 55(3), 264–271. https://doi.org/10.1093/annhyg/meq085.
(33) Howe, M.-S. (2020). The world is its own best model: Modelling and future pandemic planning in dentistry. British Dental Journal, 229(11), 716–720. https://doi.org/10.1038/s41415-020-2403-z.
(34) Eden, E., Frencken, J., Gao, S., Horst, J. A., & Innes, N. (2020). Managing dental caries against the backdrop of COVID-19: Approaches to reduce aerosol generation. British Dental Journal, 229(7), 411–416. https://doi.org/10.1038/s41415-020-2153-y.
(35) Fang, L., Karakiulakis, G., & Roth, M. (2020). Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? The Lancet Respiratory Medicine, 8(4), e21. https://doi.org/10.1016/S2213-2600(20)30116-8.
(36) Rinott, E., Kozer, E., Shapira, Y., Bar-Haim, A., & Youngster, I. (2020). Ibuprofen use and clinical outcomes in COVID-19 patients. Clinical Microbiology and Infection, 26(9), 1259.e5-1259.e7. https://doi.org/10.1016/j.cmi.2020.06.003.
(37) Joseph, R., Highton, M., & Goodrich, C. (2021). Let’s talk about scrubs: A reflection during COVID-19. Nursing Management, 52(3), 26–32. https://doi.org/10.1097/01.NUMA.0000733624.74420.43.
(38) Bar-On, Y. M., Flamholz, A., Phillips, R., & Milo, R. (2020). SARS-CoV-2 (COVID-19) by the numbers. ELife, 9, e57309. https://doi.org/10.7554/eLife.57309.
(39) Virdi, M. K., Durman, K., & Deacon, S. (2021). The Debate: What Are Aerosol-Generating Procedures in Dentistry? A Rapid Review. JDR Clinical and Translational Research, 6(2), 115–127. https://doi.org/10.1177/2380084421989946.
(40) Jacimovic, J., Jakovljevic, A., Nagendrababu, V., Duncan, H. F., & Dummer, P. M. H. (2021). A bibliometric analysis of the dental scientific literature on COVID-19. Clinical Oral Investigations. https://doi.org/10.1007/s00784-021-03916-6.