


ABSTRACT Background: Effective infection prevention and control (IPAC) practices are critical for preventing transmission of disease and maintaining population health, especially in long-term care homes (LTCHs). Canadian LTCHs rely extensively on personal support workers (PSWs) for care and IPAC implementation. However, their experiences are under-represented in IPAC programming within the LTCH settings. This study uses mixed methods to describe the perspectives of PSWs and identify factors influencing their IPAC knowledge to inform inclusive and effective IPAC implementation strategies in LTCHs.
Kathleen Qu, MSc, MPH1, Jorida Cila, PhD1*, Rhiannon Mosher, PhD1, Alexander Varsaneux, Med1, Teodora Riglea, PhD1, Keyssie Beaubrun Desinor, BSN, RN, Aboubakar Mounchili, PhD1, Tiberius Stanescu, BSN, RN, CIC, LTC-CIP2, Barbara Catt, BSN, RN, MEd, CIC, LTC-CIP, AL-CIP1, and Kanchana Amaratunga, MD, MPH, FRCPC1
1 Public Health Agency of Canada, Nepean, ON, Canada
2 Scarborough Health Network, Scarborough, ON, Canada
*Corresponding author
Jorida Cila
Public Health Agency of Canada
Nepean, ON, Canada
email: jorida.cila@phac-aspc.gc.ca
Article history:
Received 3 August 2025
Received in revised form 29 October 2025
Accepted 4 November 2025
ABSTRACT
Background: Effective infection prevention and control (IPAC) practices are critical for preventing transmission of disease and maintaining population health, especially in long-term care homes (LTCHs). Canadian LTCHs rely extensively on personal support workers (PSWs) for care and IPAC implementation. However, their experiences are under-represented in IPAC programming within the LTCH settings. This study uses mixed methods to describe the perspectives of PSWs and identify factors influencing their IPAC knowledge to inform inclusive and effective IPAC implementation strategies in LTCHs.
Methods: We surveyed a convenience sample of PSWs working in Canadian LTCHs (N = 1,166). Participants responded to a series of questions on IPAC knowledge, responsibilities, drivers, and barriers to compliance.
Results: The findings indicated strong IPAC knowledge, and the willingness to learn more about advanced topics like antimicrobials and medication side effects. Being an agency staff (third party contract employee) was associated with lower IPAC knowledge while feeling comfortable asking IPAC questions and feeling respected by colleagues were associated with higher IPAC knowledge. A shortage of personal protective equipment was not identified as a barrier to IPAC practices. Respondents identified that quality training, professional development opportunities, and supportive work environments would improve PSW engagement in IPAC.
Conclusion: This study highlights the impact of interprofessional relationships on PSW’s IPAC perceptions, knowledge, and engagement. PSWs represent the most
abundant resources in LTCHs and by bringing their experiences to light, their expertise at the frontlines can be leveraged to improve care in Canadian LTCHs.
KEYWORDS:
Mixed methods; IPAC knowledge; infection prevention and control; personal support workers; long-term care homes
INTRODUCTION
Effective infection prevention and control (IPAC) practices are critical for preventing transmission of disease and maintaining population health, especially in long-term care homes (LTCHs). LTCH residents tend to be older, have clinically complex needs, and are at higher risk of infection compared to the general population (Nicolle, 2014). During the first six months of the COVID-19 pandemic in Canada, nearly one third of LTCHs reported an outbreak (CIHI, 2023). The Canadian Institute for Health Information (CIHI) further published that the Canadian Armed Force deployed to support the most severely impacted LTCHs, reported poor IPAC practices and extensive staffing shortages in homes (CIHI, 2023).
While systemic challenges such as staffing shortages and inconsistent IPAC practices were identified, it is essential to consider the primary workforce responsible for the day-to-day resident care and IPAC implementation: personal support workers (PSWs). PSWs are non-regulated frontline staff that account for up to 60% of LTCH staff (PHO, 2018) and are responsible for up to 80% of resident care (Berta et al., 2013). Their responsibilities include assisting with activities of daily living (e.g., eating, clothing, toileting) and also clinical tasks (e.g., dressing wounds, administering medication, collecting samples for testing) (OPSWA, 2014). There is an estimated 350,000 to 2 million PSWs working in LTCHs across Canada (Zagrodney et al., 2022). PSWs constitute mostly women aged 30-50 years old, with increasing minority representation (15-42% depending on the province), face low wages, job insecurity, and role ambiguity (Kelly, 2017; Zagrodney et al., 2022). In Canada, PSW training programs average 7 months (range 3-12 months) and vary in clinical hours (ACCC, 2012). Although some provincial policies exist (PHO, 2018), no national regulation exists to ensure consistent PSW education nor role definition (Kelly, 2017). PSW demand and workloads are rising with an aging population and growing healthcare costs (Zagrodney & Saks, 2017). These factors shape the working conditions and PSWs’ capacity to engage in
IPAC effectively.
Adherence to IPAC practices among healthcare professionals has been widely studied, with a 2020 Cochrane review highlighting how organizational (e.g., management support, training), environmental (e.g., facility design, supply availability), and individual (e.g., beliefs and attitudes) factors all influence uptake (Houghton et al., 2020). These findings emphasize that IPAC is shaped not only by individual knowledge but also by broader systemic and workplace conditions. Specific to PSWs, two recent Canadian studies have underscored their critical role in IPAC and the challenges they face in maintaining best practices. An Ontario study involving 326 PSWs highlighted PSW staffing challenges were fuelled by existing staff shortages, organizational issues (management support), resident and family pressures, and systemic issues (stigma and disrespect) (CLRI, 2021). In British Columbia (BC), a survey of 441 PSWs (known as “healthcare workers” in BC) found that IPAC adherence could be strengthened through stronger leadership, enhanced training, and improved personal protective equipment (PPE) access (Srigley et al., 2023). While informative, these studies were provincial in scope and did not capture the perspectives of PSWs nationwide.
PSWs are indeed underrepresented in IPAC programming within Canadian LTCHs. As a result, the valuable expertise and frontline experiences of this major group of care providers are not being fully leveraged to inform and improve IPAC strategies in these settings. This study uses mixed methods to describe the perspectives of PSWs and identify factors influencing their IPAC knowledge to inform inclusive and effective IPAC implementation strategies in LTCHs.
METHODS
The survey development was informed by a literature review and open-ended interviews with a convenience sample of 24 PSWs working in Ontario LTCHs to focus the survey on PSWs’ general perspectives, covering training needs, professional values, and interprofessional relationships. The survey included questions on demographics (e.g., age, education, employment status), knowledge, perspectives, and barriers associated with IPAC practices and an open-ended question. The survey was piloted by 13 PSWs and further revised based on the feedback.
Knowledge
This section assessed PSWs’ knowledge, attitudes, and work-related behaviours. This included what topics would be of interest for learning (such as antimicrobial resistance (AMR), medication side effects, and others). Two sets of true/false questions based on the Canadian Standards Association guidelines assessed knowledge of IPAC best practices
(e.g., “Gloves can be used instead of practicing hand hygiene.”) (CSA, 2022).
Perspectives
Respondents used a 5-point Likert scale to rate their confidence in completing activities expected of PSWs (e.g., use of PPE) and teaching others about IPAC. Participants also indicated their perception of IPAC responsibility among various LTCH staff, level of comfort asking IPAC questions, and attitudes towards IPAC practices.
Barriers
Questions assessed PSWs’ perceived barriers to practicing IPAC (5-point Likert scale), and views on various IPAC practices associated with leadership opportunities and
time constraints.
The nation-wide survey included self-identified PSWs currently working in a Canadian LTCH. Informed consent for voluntary participation was obtained and no incentive for participation was provided. The project involved minimal risk to participants; no additional ethics approval was required. Participants were briefed on data confidentiality practices and informed only summary results would be published. The online survey was accessible in English and French on Qualtrics from August 8 to October 13, 2023,
with the survey link shared by distribution partners, including Canadian Support Workers’ Association and Infection Prevention and Control Canada and attempting to reach approximately 80,000 PSW members across Canada.
Descriptive analysis was conducted to report proportions, means and confidence intervals for knowledge scores. Model variable selection was informed by theoretical framework insights and univariate analysis at liberal p < 0.1 threshold. A multivariate linear regression model was then used to model variables associated with IPAC knowledge (p<0.01). Non-linear relationships were considered when model findings diverged from theoretical framework and expert experience. Model diagnostics and analyses were performed in R 4.4 (R, 2024) and Microsoft Excel (Microsoft, 2024).
Open-ended responses were analyzed thematically by two coders with experience in LTCHs and behavioural science (Braun & Clarke, 2006). Discrepancies between coders were resolved through team discussions. Qualitative and quantitative results were reviewed together to identify patterns, linking findings to the theoretical framework
and literature.
RESULTS
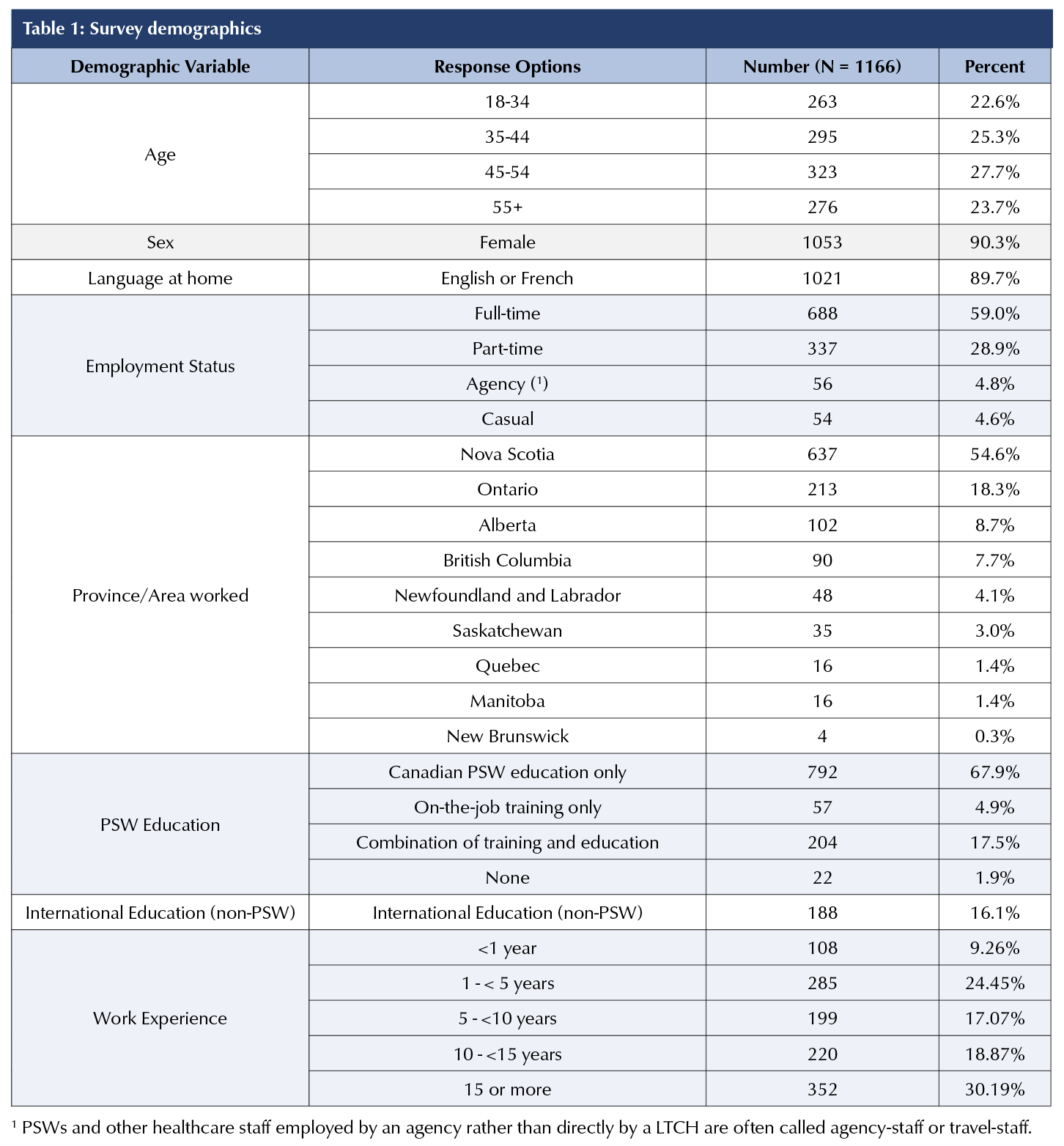
The final sample included 1,166 respondents: 90.3% female, 58% were 34-54 years old; 89.7% spoke English or French at home, and 54.6% worked in Nova Scotia (Table 1). Most respondents had Canadian PSW education (67.9%). Of those with Canadian training, 91.6% completed PSW programs that were at least six months long. Among the internationally trained respondents (16.1%), 59% had nursing training. One-third of respondents had ≥15 years of PSW experience and 90.2% only had work experience in LTCHs. Fewer than 10% worked for an agency or casually (Table 1).
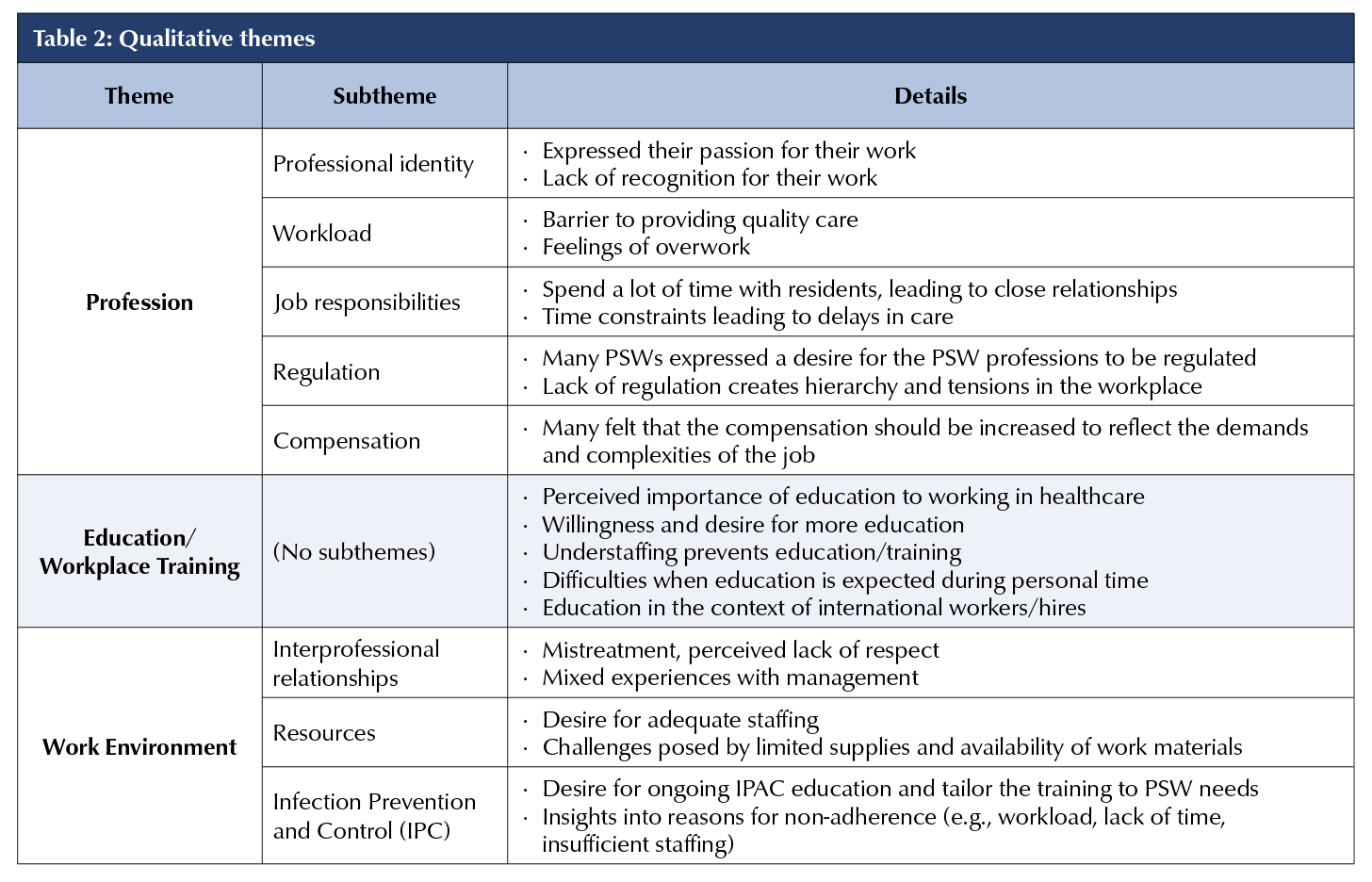
Twenty-seven percent (316/1166) submitted open-ended question responses, revealing three key themes: 1) insights into PSW profession; 2) experiences and suggestions for education and workplace training; and 3) work environment considerations (Table 2).
Knowledge
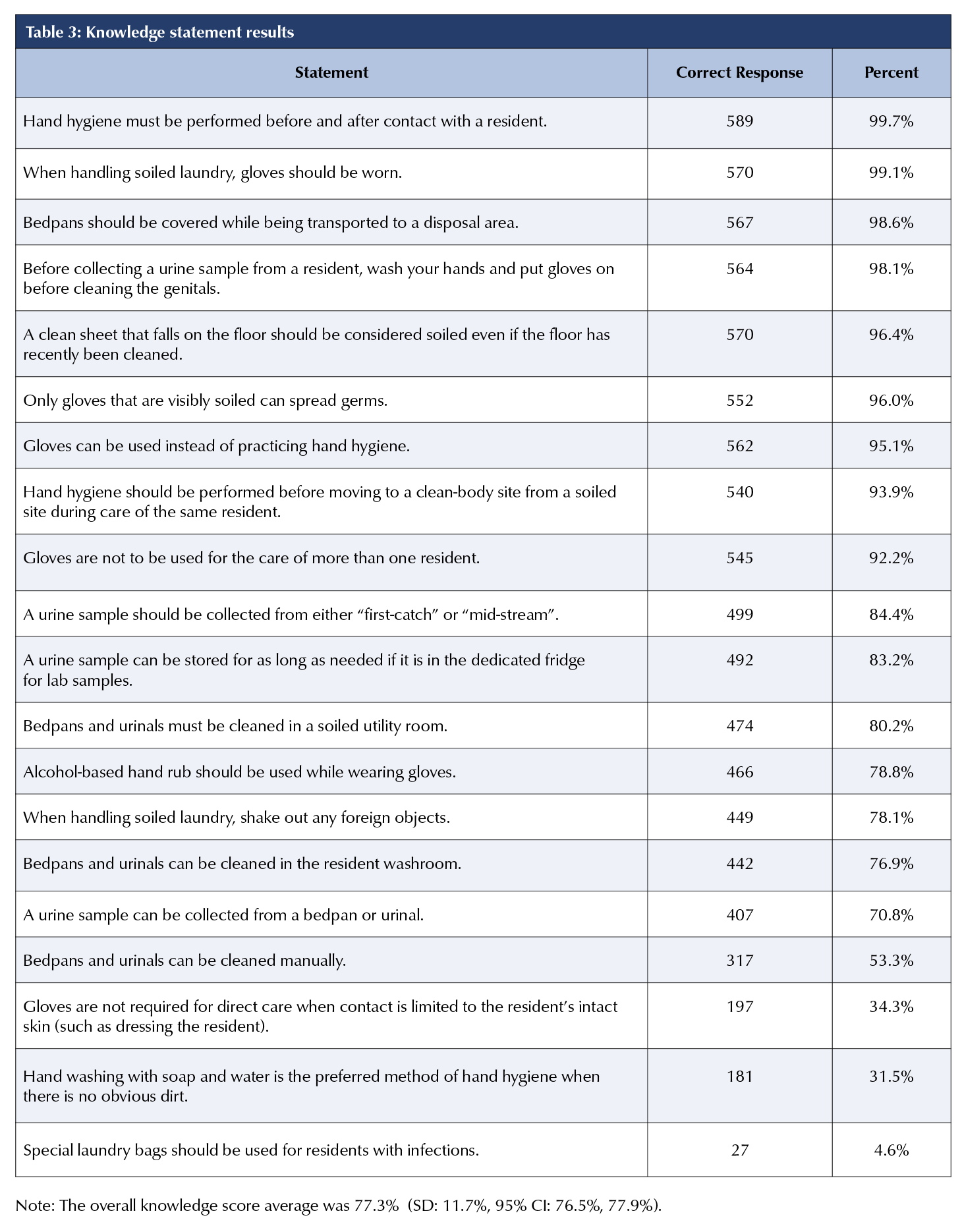
No statistically significant difference was observed when comparing the two sets of IPAC knowledge questions (Wilcoxon test p = 0.7) and so were combined for analysis (M= 77.3%, SD = 11.7%). Most correct answers were related to hand hygiene. However, two related questions only received correct responses from one-third of participants. Most incorrect answers were to a question on special laundry bag use (Table 3).
PSWs reported varied levels of IPAC training, from none (25.9%) to only during outbreaks (23.9%), and ongoing but less frequently than monthly (20.8%). Most PSWs preferred group training sessions (61.6%), specifically in-person, whereas 10.4% had no preferences. Almost half of respondents (45.2%) preferred IPAC training once a month; 12.9% had no preferences, and 1.5% did not want training.
Respondents expressed desire for leadership roles and support for additional professional development. Over 90% of respondents have learned about PPE use while many expressed interests in learning about AMR (80.7%), IPAC leadership opportunities (69.4%), and antimicrobial stewardship (69%). Many respondents shared their willingness and desire for more educational activities, underscoring its importance to their role:
“IPAC training should be frequent and ongoing. Many staff confuse [COVID-19] isolation with other types of isolation and are unsure how to protect the resident and themselves. New staff can quickly forget their IPAC training, as they have so many new things to remember in their first few weeks as a new employee.”
In open-ended responses, some participants described training – such as annual hand hygiene sessions – as repetitive, however IPAC knowledge scores identified gaps in hand hygiene continue to persist. A concern may be the quality of training or time allotted for training as only 27.6% reported compensation for any training:
“Most education is left to our own efforts, unpaid, online except for the few things that require a daylong session, which we are paid but must go on our day off to attend.”
Perspectives
Most respondents reported high confidence in carrying out IPAC activities. Over 90% of respondents had confidence in practicing hand hygiene, but only half were confident in providing IPAC education to other PSWs or residents. Respondents recognized IPAC’s importance in protecting everyone’s health (95%). Most agreed it was an important aspect of PSWs’ role (93.3%), with over 90% indicating PSWs were equally responsible for IPAC as nurses and designated IPAC staff. Respondents felt most comfortable asking IPAC questions to nurses (78.6%), followed by designated IPAC staff (69.3%). Less than half (47.1%) were comfortable asking another PSW and 3% did not feel comfortable asking anyone. Over half (54.8%) strongly agreed or agreed that they were willing to take on IPAC leadership roles.
Barriers and drivers
Time constraints were a persistent barrier to practicing IPAC. One third (31%) of respondents indicated not having enough time to complete required IPAC best practices during their shift, whereas 47.3% lacked capacity to take on IPAC leadership roles despite showing interest. Open responses added that heavy workloads limited care quality and personal well-being for themselves and residents. Notably, 81.1% indicated PPE shortage was not a barrier to IPAC practices.
Over half (56.2%) of respondents felt they often had IPAC support in the form of someone answering their questions, IPAC learning sources (56.3%), or sufficient training (55.6%). PPE was often or very often available for most respondents (81.1%). More than three quarters (76.9%) felt they always or often had enough information to provide the best care to the residents.
Respondents frequently discussed interprofessional relationships and the perceived value of PSWs role. Only half of respondents felt included in conversations about residents’ care plans or felt respected by registered and non-registered staff. Open comments reflected these diverse experiences, ranging from experiences of strong management support and involvement in resident care to feeling disrespected, unrecognized, ostracized for openly sharing their concerns, or disconnected from administrators (e.g., who only communicated via email):
“I feel very involved in the care of the residents at the facility I work at. There are endless education programs to boost your knowledge and allow you to make the best decisions possible for the people I am caring for. Management is always available
to ask questions to and provide support. I have been a [PSW] at [my LTCH] for 10 years.”
“I feel as a [PSW] we are left out of a lot of things, and we need to be more involved because we are the primary care of residents.”
“I’m not comfortable asking questions where I work because I have been called a troublemaker.”
Only 21.9% of respondents identified having IPAC leadership opportunities at work. Even in a leadership role, some reported their expertise being challenged:
“I have been a member of our IPAC committee at the LTC facility that I work. Although I am well respected as a PSW at the facility by all staff, I wasn’t [received] well as a member of the team […] when I brought valid complaints or problems that [I] received from other [workers] to the IPAC team some were implemented but most were brushed over or ignored […] Registered staff do not respect their opinion and fellow staff see them as ‘snitches’.”
Many PSWs took the survey as an opportunity to share their strong sense of professional identity, passion and commitment despite daily challenges. One shared that being “a [PSW] is such a rewarding job” but one that is often “very difficult” due to short staffing and limited supplies. Some suggested PSW regulation may be beneficial to uphold professional and care standards.
Modelling IPAC knowledge
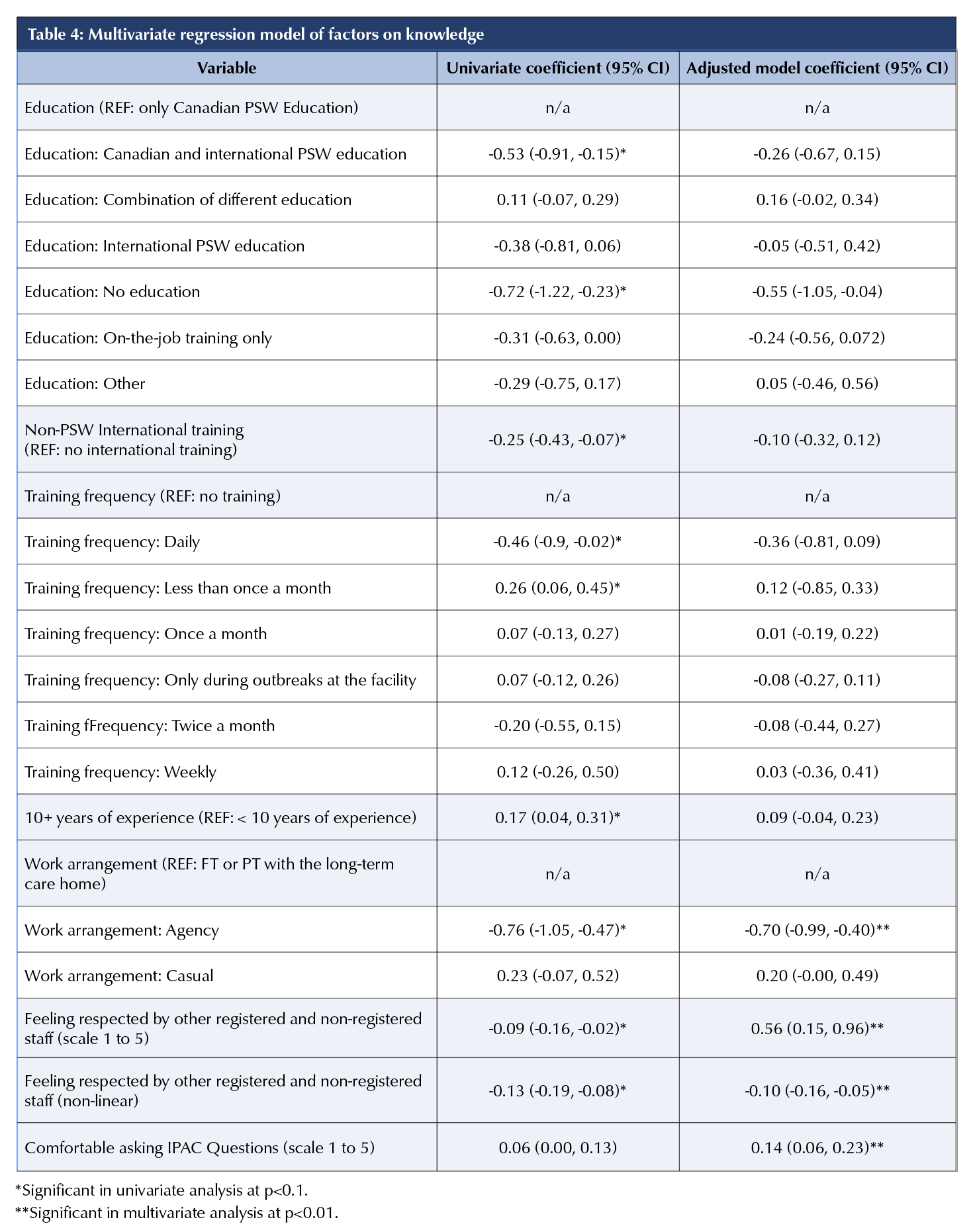
A multivariate linear regression was used to identify variables associated with IPAC knowledge (Table 4). Feeling respected and having access to IPAC support had theoretical importance and were therefore included in the model. In the adjusted model, agency-employed PSWs were more likely to have lower IPAC knowledge compared to PSWs employed full- or part-time by a LTCH. This was also emphasized in the write-in responses:
“The travel staff that have come into our facility were given zero training and [go] all throughout the building with full personal protective equipment on. Travel staff are not washing their hands in between residents at any level of care being done.”
There was a statistically significant nonlinear relationship between feeling respected by staff and stronger knowledge (Table 4). Greater comfort asking IPAC questions was associated with higher IPAC knowledge. Internationally educated PSWs did not have a statistically significant difference in IPAC knowledge compared to domestically educated PSWs.
DISCUSSION
PSWs are vital in LTCHs, but their perspectives are underrepresented in IPAC program implementation. Building on the existing literature, this study provides insight on IPAC implementation to leverage PSWs’ expertise by focusing on barriers and drivers influencing PSWs’ IPAC knowledge and practices.
The study findings underscore the role of interprofessional relationships in PSWs’ perceptions, knowledge, and engagement in IPAC practices. Half of respondents reported not feeling respected by colleagues and management. Feeling comfortable asking IPAC questions was directly associated with better IPAC knowledge. Respondents flagged interprofessional tensions, including deteriorating trust and lack of peer knowledge sharing, as detrimental to IPAC engagement. Reliance on agency staff has been previously associated with decreased quality of care (Office of the Auditor General of Ontario, 2023), a concern that also surfaced in this study with a notable difference in IPAC knowledge and tension related to inconsistent education and care quality between LTCH staff and agency staff. Additionally, some respondents from Nova Scotia identified that the provincial certification program provided monetary incentives that unintentionally devalued the professional experience and knowledge of long-serving PSWs’ professional experience and knowledge. These complex relationships among PSWs and their peers and other healthcare professionals significantly impact IPAC implementation and the PSWs’ workflow. Equally important, the study identified that feeling comfortable asking IPAC questions and feeling respected were associated with better IPAC knowledge outcomes. This finding suggests interprofessional relationships should be prioritized as it is a significant factor and opportunity for improving IPAC engagement in LTCHs among PSWs.
Echoing the findings in BC (Srigley et al., 2023), PSWs in this study desired effective, tailored IPAC training for enhancing competencies. Contrary to previous reports (CIHI, 2023, Srigley et al., 2023), many were not concerned with PPE shortage as a barrier to IPAC practices. Gaps in hand hygiene and glove use knowledge may not be directly attributable to education, but could stem from organizational barriers, workplace cultural norms, incorrect training, or lack of awareness of microorganism transmission (Kristiansen et al., 2024; PHAC, 2012).
Effective training comes from creating more opportunities to learn, and ask questions on topics of interest. We found that PSWs expressed interest in training on IPAC leadership, AMR, antimicrobial risks, and antimicrobial side effects (Andersen, 2009; Kelly, 2017). Respondents preferred monthly in-person group training over other formats which can be associated with better peer-support and a conducive learning environment. Promoting best practices requires in-depth training that recognizes organizational barriers and the local context (Cheng et al., 2024).
Although demonstrated interest in IPAC leadership opportunities, many faced organizational and individual barriers, including lack of time, lack of training, and low self-confidence. Professional standardization can support PSWs professionally and leverage existing resources to uphold IPAC standards (Belan et al., 2020; CIHI, 2023b; IPAC LTCH Interest Group, 2021). PSW roles are typically dictated by local LTCH’s needs rather than PSWs’ competencies, thus contributing to lack of leadership opportunities, and inadequate professional development. LTCHs and policymakers can collaborate with groups such as the Canadian Support Workers’ Association to define responsibilities to better leverage PSWs as assets for peer education, resident education, and IPAC leadership (PHO, 2018; Savendranayagam et al., 2021).
The survey was limited in representation across all types of PSWs working in the LTCH setting across Canada, resulting in considerable selection bias. Most respondents spoke English or French at home, suggesting a significant immigrant population known in the PSW workforce may not be represented (Zagrodney et al., 2022). Additionally, due to disproportionate representation, no provincial stratification was possible. Representation from agency staff was also limited. Only a subsample responded to open-ended questions, limiting generalizability of the thematic findings. Anonymity prevented follow-up questions for deeper interpretation of text responses.
CONCLUSION
PSWs are essential to LTCHs and play a key role in IPAC, however, they continue to be under-represented in IPAC literature beyond implementation. This is the first national study to position their expertise and experience to improve IPAC in LTCHs using a mixed methods approach. PSWs are committed to quality care, with many eager to expand their professional competencies in IPAC leadership and related topics such as AMR. Enhancing interprofessional relationships, providing quality training, and professional regulation can better position PSWs to carry out IPAC best practices and take on leadership roles within LTCHs. There is growing research, scrutiny, and demand for improvement of care in LTCHs across Canada and an important step towards successful programming includes bringing PSWs into quality improvement projects not only as subjects but as experts and primary care providers in LTC settings.
REFERENCES
Andersen, E. A. (2014). Working in long-term residential care: A qualitative meta summary encompassing roles, working environments, work satisfaction, and factors affecting recruitment and retention of nurse aides.
Global Journal of Health Science, 1(2).
https://doi.org/10.5539/gjhs.v1n2p2
Belan, M., Thilly, N., & Pulcini, C. (2020). Antimicrobial stewardship programmes in nursing homes: A systematic review and inventory of tools. Journal of Antimicrobial Chemotherapy, 75(6), 1476–1488.
https://doi.org/10.1093/jac/dkaa013
Berta, W., Laporte, A., Deber, R., Baumann, A., & Gamble, B. (2013). The evolving role of health care aides in the long-term care and home and community care sectors in Canada. Human Resources for Health, 11, 25.
https://doi.org/10.1186/1478-4491-11-25
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
Canadian Institute for Health Information. (2023a). Recommendations for advancing pan-Canadian
data capture for personal support workers.
Ottawa, ON: Author.
https://www.cihi.ca/sites/default/files/document/recommendations-advancing-pan-canadian-data-capture-psws-report-en.pdf
Canadian Institute for Health Information. (2023b). Long-term care and COVID-19: The first 6 months.
https://www.cihi.ca/en/long-term-care-and-covid-19-
first-6-months
Canadian Standards Association. (2022). Long-term care home operations and infection prevention and control. Ottawa, ON: Author.
Centres for Learning, Research and Innovation. (2021). PSW perspectives on the staffing challenge in long-term care: Final report.
https://clri-ltc.ca/files/2021/02/PSW_Perspectives_FinalReport_Feb25_Accessible.pdf
Cheng, B. T., Ali, R. A., Chen Collet, J., Donovan Towell, T., Han, G., Keen, D., … Srigley, J. A. (2023). Barriers to healthcare-worker adherence to infection prevention
and control practices in British Columbia during the coronavirus disease 2019 (COVID-19) pandemic:
A cross-sectional study. Infection Control & Hospital Epidemiology, 45(4), 474–482.
https://doi.org/10.1017/ice.2023.242
Houghton, C., Meskell, P., Delaney, H., Smalle, M., Glenton, C., Booth, A., Chan, X. H. S., Devane, D., & Biesty, L. M. (2020). Barriers and facilitators to healthcare workers’ adherence with infection prevention and control (IPC) guidelines for respiratory infectious diseases: A rapid qualitative evidence synthesis. The Cochrane Database of Systematic Reviews, 4, CD013582. https://doi.org/10.1002/14651858.CD013582
IPAC Canada Long-Term Care Interest Group. (2021). Position statement: Infection prevention and control program components for long-term care homes. Canadian Journal of Infection Control, 125–128.
https://cjic.ca/fall-2021/298-position-statement-infection-prevention-and-control-program-components-for-long-term-care-homes
Kelly, C. (2017). Exploring experiences of personal support worker education in Ontario, Canada. Health & Social Care in the Community, 25(4), 1430–1438.
https://doi.org/10.1111/hsc.12443
Kristiansen, P. C., Bastien, S., Debesay, J., & Fagernes, M. (2024). How and why do healthcare workers use gloves in two Norwegian nursing homes? The Journal of Hospital Infection, 146, 134–140.
https://doi.org/10.1016/j.jhin.2024.02.005
Microsoft Corporation. (n.d.). Microsoft Excel
[Computer software].
Nicolle, L. E. (2014). Antimicrobial stewardship in long-term care facilities: What is effective? Antimicrobial Resistance and Infection Control, 3, 6.
https://doi.org/10.1186/2047-2994-3-6
Ontario Personal Support Worker Association. (2014). In PSW scope of practice (Ed.). Ontario, Canada: Author. https://4fb5d6bf-32bd-43e7-82da-f0da7f451b7f.filesusr.com/ugd/207a84_b03b2bf53e974fb397176b3c02e91da2.pdf
Office of the Auditor General of Ontario. (2023). Annual report on long term care and residential services 2023.
https://www.auditor.on.ca/en/content/annualreports/arreports/en23/AR_LTCresidential_en23.pdf
Public Health Agency of Canada. (2012). Hand hygiene practices in healthcare settings.
https://publications.gc.ca/collections/collection_2012/aspc-phac/HP40-74-2012-eng.pdf
Public Health Ontario. (2018). Antimicrobial stewardship essentials in long-term care: Antimicrobial stewardship as quality improvement. Ontario, Canada: Queen’s Printer for Ontario.
https://www.publichealthontario.ca/-/media/documents/p/2018/primer-antimicrobial-stewardship-ltc.pdf?sc_lang=en
R Core Team. (2024). R [Computer software]. Vienna, Austria.
Savundranayagam, M. Y., Docherty-Skippen, S. M., & Basque, S. R. (2021). Qualitative insights into the working conditions of personal support workers in long-term care in the context of a person-centered communication training intervention. Research in Gerontological Nursing, 14(5), 245–253. https://doi.org/10.3928/19404921-20210708-01
Srigley, J. A., Cheng, B., Collet, J. C., Donovan Towell, T., Han, G., Keen, D., Leung, K. W., Mori, J., & Ali, R. A. (2023). Barriers to infection prevention and control in long-term care/assisted living settings in British Columbia during the COVID-19 pandemic: A cross-sectional survey. Antimicrobial Resistance and Infection Control, 12, 84. https://doi.org/10.1186/s13756-023-01292-2
The Association of Canadian Community Colleges, & Canadian Association of Continuing Care Educators. (2012). Canadian educational standards for personal care providers.
https://cacce.ca/wp-content/uploads/2021/11/Reference-Guide_Canadian-Educational-Standards-for-Personal-Care-Providers_ACCC.pdf
Zagrodney, K., Deber, R., Saks, M., & Laporte, A. (2022). Personal support worker socio-demographic differences across care sectors in Canada. Journal of Applied Gerontology, 42(4), 670–679.
https://doi.org/10.1177/07334648221142301
Zagrodney, K., & Saks, M. (2017). Personal support workers in Canada: The new precariat? Healthcare Policy, 13(2), 31–39. https://doi.org/10.12927/hcpol.2017.25324